Introduction
Imagine waking up after a full night’s sleep, yet feeling as though you haven’t slept in days. Your limbs feel heavy, as if you are moving through molasses, and the mental effort required to simply plan your day feels akin to solving complex calculus.
This is not the “tiredness” that follows a long day of work or a rigorous gym session. This is Parkinson’s disease (PD) fatigue—a symptom that is as enigmatic as it is debilitating.
For decades, the public focus on Parkinson’s has centered on the visible motor symptoms: the tremors, the stiffness, and the shuffling gait.
However, for those living with the condition, the reality is often quite different. Studies consistently show that fatigue affects between 33% and 81% of patients, with nearly one-third citing it as their single most disabling symptom. It is an overwhelming sense of exhaustion that encompasses both physical and mental domains, often disproportionate to the activity undertaken and frequently unalleviated by rest.
Crucially, fatigue is not a sign of laziness, depression, or a simple lack of sleep. It is a primary physiological manifestation of the disease itself—a signal that the neurodegenerative process is affecting networks far beyond those that control movement.
By peeling back the layers of neurobiology, inflammation, and metabolic failure, we can begin to validate this invisible struggle and, more importantly, find strategic ways to manage it. This article explores the deep science behind why fatigue occurs and offers evidence-based strategies to reclaim your energy.
Fatigue: More Than Just Being “Tired”
To manage fatigue, we must first define it accurately. In the clinical landscape of Parkinson’s, fatigue is a distinct entity, separate from sleepiness (somnolence) or a lack of interest (apathy), though they often overlap.
Fatigue in PD is multidimensional. Patients often describe a “failure to initiate”—a sensation where the brain knows what to do, but the body simply cannot muster the energy to execute the command. This is known as Subjective Fatigue. It is a central sensation, a perception of weariness that acts as a heavy cloak over daily life.
Interestingly, this internal feeling doesn’t always match muscle performance. You might feel too weak to walk, but your muscles are physiologically capable of the task.
Contrast this with Objective Fatigability, which is a measurable decline in performance. In PD, this is “peripheral” fatigability. If you were to perform a repetitive motion, your force generation would decline more rapidly than that of a healthy person. This creates a frustrating disconnect: a central nervous system that struggles to drive the muscle, combined with muscles that tire too quickly.
Furthermore, the fatigue is pleiotropic, meaning it affects multiple systems. There is Physical Fatigue, characterized by muscle weakness and kinetic exhaustion, and Mental Fatigue, a difficulty in sustaining attention or concentration.
The latter is particularly intrusive, making tasks that require executive function—like balancing a checkbook or following a conversation—feel like climbing a mountain.
Understanding these distinctions is the first step toward targeted management.

The Science Behind Fatigue in Parkinson’s
Why does the brain stop generating energy?
One of the most compelling neurobiological theories is the Effort-Reward Imbalance Hypothesis.
Every action we take, from reaching for a coffee cup to walking to the mailbox, involves a split-second calculation by the brain: Is the reward of this action worth the effort required to achieve it? This calculation relies heavily on dopamine, particularly in the mesolimbic system—the brain’s reward center.
In Parkinson’s, the degeneration of dopamine-producing neurons isn’t limited to the areas controlling movement (the nigrostriatal pathway). It extends to the ventral tegmental area, which projects to the nucleus accumbens. When dopamine is depleted here, the brain’s “currency converter” breaks down.
The result is a skewed cost-benefit analysis. The brain begins to inflate the perceived “cost” (effort) of an action while diminishing the perceived “value” of the reward. To the PD brain, walking to the kitchen might “cost” as much energy as running a mile, while the reward of getting a glass of water feels negligible.
Consequently, the sensation of fatigue acts as a behavioral “stop signal.” It is the brain’s misguided attempt to conserve energy because it calculates that the exertion isn’t justified. This “central activation deficit” means patients have to exert massive mental willpower to override this stop signal, leading to profound exhaustion.
Additionally, this isn’t just about dopamine. Serotonin, the neurotransmitter regulating mood and sleep, plays a massive role. Serotonergic neurons in the brainstem often degenerate before dopamine neurons. PET scan studies reveal that fatigued PD patients have significantly reduced serotonin transporter availability in the limbic system.
This explains why fatigue often persists even when patients are perfectly medicated with Levodopa—the dopaminergic deficit is treated, but the serotonergic “non-dopaminergic” fatigue remains.
Inflammation and “Sickness Behavior”
While the brain struggles with neurotransmitters, the body is fighting its own battle. Emerging research supports a “whole-body” view of PD fatigue, suggesting it mimics “sickness behavior”—the lethargy you feel when you have the flu.
Parkinson’s is increasingly viewed as a state of chronic, low-grade inflammation. Patients often exhibit elevated levels of pro-inflammatory cytokines, specifically Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-alpha). These inflammatory messengers don’t just stay in the blood; they cross the blood-brain barrier and activate microglia, the brain’s immune cells.
When microglia are activated, they release reactive oxygen species and more cytokines, creating a toxic, inflammatory environment that impairs neural signaling. This biological state signals the body to withdraw, rest, and conserve energy to “fight” an infection that isn’t actually there.
A key player in this process is the NLRP3 inflammasome, an intracellular alarm system. In a healthy brain, dopamine inhibits this alarm. But in PD, as dopamine levels fall, the “brake” on the immune system is removed. The NLRP3 inflammasome becomes hyperactive, churning out inflammatory signals that drive fatigue.
Simultaneously, there is a crisis in the cellular power plants: the mitochondria. A systemic reduction in Complex I activity of the mitochondrial electron transport chain is a robust finding in PD. This means the cells are literally less efficient at producing ATP, the energy currency of life. This bioenergetic failure is systemic, found in skeletal muscles as well as the brain, explaining why physical endurance is so compromised.
Factors Contributing to Fatigue
If neurodegeneration and inflammation are the core of the onion, secondary comorbidities are the outer layers. These are often the most treatable aspects of fatigue, yet they frequently go diagnosing.
Sleep Pathology is ubiquitous. It’s not just about getting eight hours; it’s about the quality of that sleep. Many PD patients suffer from Obstructive Sleep Apnea (OSA) or REM Sleep Behavior Disorder (RBD), where they physically act out dreams. This fragmentation prevents restorative sleep, leaving the brain in a permanent state of debt.
Autonomic Dysfunction is another silent thief of energy. Many patients experience Neurogenic Orthostatic Hypotension (nOH)—a drop in blood pressure upon standing. This happens because the autonomic nervous system fails to release enough norepinephrine to constrict blood vessels. The result is chronic cerebral hypoperfusion. Even if you don’t faint, your brain is getting slightly less oxygen than it needs whenever you are upright. This manifests as “brain fog,” visual blurring, and a coat-hanger ache in the neck and shoulders—all perceived as profound tiredness.
Finally, we must address Neuropsychiatric Factors. While depression and fatigue are distinct, they feed into each other. Depression can rob a patient of motivation (anhedonia), while apathy—a lack of interest separate from sadness—can mimic the “effort-reward” failure of fatigue. Distinguishing these requires careful clinical assessment, as the treatment for depression (SSRIs/SNRIs) differs from the treatment for pure fatigue or apathy.

Pharmacological Management: Consult Your Doctor
When it comes to treating fatigue with medication, the landscape is complex and highly individualized. There are numerous pharmaceutical options available today that target different aspects of fatigue—whether it stems from dopamine deficiency, excessive daytime sleepiness, or other underlying chemical imbalances.
However, because fatigue in Parkinson’s is so multifaceted—involving everything from neurotransmitters to blood pressure regulation—no single drug works for everyone.
What provides energy for one patient might cause side effects in another.
Therefore, it is absolutely essential to have a detailed conversation with your neurologist or movement disorder specialist. They can help identify the specific type of fatigue you are experiencing and tailor a treatment plan that is safe and effective for your unique medical profile.
Exercise: The Only Disease-Modifying Strategy?
While pills treat symptoms, exercise may actually change the biology of the fatigued brain. It is arguably the most robust intervention available.
Aerobic Training is critical. Regular cardiovascular exercise (walking, cycling, swimming) does more than just strengthen the heart; it lowers the resting levels of those pro-inflammatory cytokines (IL-6) that drive sickness behavior. It also improves oxygen delivery to the mitochondria, helping to mitigate the bioenergetic failure.
However, intensity matters. Emerging research on High-Intensity Interval Training (HIIT) suggests that pushing your heart rate to 60-80% of its reserve triggers the release of Brain-Derived Neurotrophic Factor (BDNF). BDNF acts like fertilizer for the brain, promoting synaptic plasticity in the basal ganglia. High-intensity work has also been shown to normalize “cortical silent periods”—essentially resetting the excitability of the motor cortex.
Resistance Training is the other half of the equation. By increasing muscle strength, you lower the relative effort required for daily tasks. If your legs are stronger, standing up from a chair takes 30% of your maximum effort instead of 80%, leaving you with more energy in the tank for the rest of the day.
The recommended prescription is a mix: at least 3 days a week of aerobic activity combined with resistance training, totaling 30-40 minutes per session.

Diet and Lifestyle Management
Finally, management extends to how you fuel your body and how you spend your energy budget.
From a dietary perspective, metabolic therapies are gaining traction. A randomized trial comparing a Mediterranean diet to a Ketogenic diet found that while both improved health, the Ketogenic group (high fat, low carb) saw significantly greater improvements in non-motor symptoms like fatigue.
The theory is that ketone bodies can bypass the defective Complex I in the mitochondria, providing an alternative, more efficient fuel source for neurons. While a strict Keto diet is hard to maintain, moving toward a lower-carb, healthy-fat diet may offer benefits.
Fatigue in Parkinson’s is a heavy burden, impacting not just the patient but the entire family unit. It limits social interaction and increases caregiver strain.
But by recognizing it as a physiological storm—of inflammation, neurochemistry, and metabolism—we can stop blaming ourselves and start managing our biology.
Through a combination of smart medication, high-intensity movement, and strategic energy budgeting, vitality is not a thing of the past.
Understanding Parkinson’s is a journey of continuous discovery. To stay updated on the latest news, insightful information, and updates regarding Parkinson’s research and management follow @photopharmics_ on social media.
Introduction
If you’re living with Parkinson’s disease (PD), you might have a deeply personal understanding of what fatigue truly means.
It’s a feeling that goes far beyond the simple tiredness you might experience after a long day.
Many describe it in profound terms: an “unrelenting and non-ending tiredness,” a “total absence of energy,” or a sensation so overwhelming it feels “impossible to move.”
This isn’t just being tired; it’s a pervasive, profound exhaustion that sleep doesn’t seem to touch.
If this sounds familiar, please know you are not alone, and what you’re experiencing is very real.
Fatigue is one of the most common and challenging non-motor symptoms of Parkinson’s, affecting more than half of all individuals with the condition.
For nearly a third of people with PD, it is their single most disabling symptom—often rated as more burdensome than the more visible motor symptoms like tremors or stiffness.
It can appear early, sometimes even before a diagnosis, and its impact on quality of life is immense, affecting work, hobbies, and the simple joy of connecting with loved ones.
This exhaustion can also bring an emotional weight. Many people with PD feel misunderstood, sometimes labeled as “lazy” or “apathetic” when, in reality, they are battling a legitimate, physiological symptom of their condition.
This article is designed to be your comprehensive guide to understanding Parkinson’s-related fatigue. We’ll explore what it is, where it comes from, and most importantly, provide some strategies to potentially help you manage your energy and reclaim your life.

Understanding Parkinson’s Fatigue: More Than Just Being Tired
To effectively fight back against fatigue, we first need to define our opponent.
Parkinson’s-related fatigue is a complex symptom, and recognizing its unique characteristics is the first step toward managing it.
What is PD-Related Fatigue?
In clinical terms, Parkinson’s fatigue is a profound sense of physical or mental exhaustion that isn’t reliably improved by rest. It’s an unpleasant feeling of lacking the energy to perform routine activities.
This exhaustion can show up in two main ways, either separately or together:
- Physical Fatigue: This is a deep weariness in your body. You might feel “run down,” like you’ve completely run “out of gas,” or as if your limbs are made of lead. This feeling can often intensify during “off” periods when your medication’s effects are wearing off.
- Mental (Cognitive) Fatigue: This is a kind of “brain fog.” It makes it difficult to concentrate, pay attention for extended periods, or even find the mental energy to start a project. It’s a feeling of mental sluggishness that can be just as debilitating as physical exhaustion.
Fatigue vs. Sleepiness vs. Apathy vs. Depression
One of the biggest hurdles in getting the right help for fatigue is that the word “tired” can mean so many different things. Let’s clear up the confusion, because telling these states apart is critical for finding the right solutions.
- Fatigue vs. Sleepiness: This is the most important distinction. Fatigue is a lack of energy, while sleepiness is the need to sleep. Someone with fatigue feels utterly exhausted but may not feel drowsy or able to fall asleep. While sleep problems are common in PD and definitely make fatigue worse, sleepiness is usually relieved by a nap. Fatigue, on the other hand, often lingers even after rest.
- Fatigue vs. Apathy: Apathy is a lack of motivation or interest. A person experiencing apathy might not want to engage in an activity. In contrast, a person with fatigue often desperately wants to do things but feels they simply don’t have the physical or mental fuel in the tank.
- Fatigue vs. Depression: There’s a significant overlap here, as fatigue is a core symptom of depression. However, many people with Parkinson’s experience severe fatigue without being clinically depressed. Treating depression can certainly improve fatigue if they coexist, but it may not eliminate the fatigue that stems directly from the disease itself.
The Pervasive Impact on Daily Life
The ripple effects of fatigue are far-reaching. It’s an unpredictable symptom that can make planning your life feel impossible. Simple tasks can become monumental efforts.
You might start a project, only to find your energy depleted after just 15 minutes. To avoid this crash, you might start avoiding activities you once loved, leading to social isolation and physical deconditioning.
This creates a “fatigue hangover,” where the exertion of one day can leave you drained for several days to follow, stripping the pleasure from life’s most meaningful moments.

The “Why”: The Causes of Fatigue
So, where does this profound exhaustion come from? The answer is complex. Fatigue in Parkinson’s isn’t caused by a single factor but by an intricate web of primary and secondary contributors.
Primary Fatigue:
For many, fatigue is a primary symptom of Parkinson’s, meaning it’s a direct result of the changes happening in the brain. It’s not just a reaction to other symptoms. The neurodegenerative process in PD affects more than just dopamine; it disrupts other neurotransmitter systems, like serotonin, which are closely linked to energy and arousal. This is why fatigue can appear so early in the disease and why its severity doesn’t always match the severity of motor symptoms.
Secondary Contributors:
On top of being a primary symptom, fatigue is often amplified by a host of secondary factors:
- The Sheer Effort of Movement: The motor symptoms of PD are physically draining. Constant tremors, the muscle rigidity that forces you to work against your own body, and the slowness of movement (bradykinesia) all demand an enormous amount of energy for even the simplest tasks.
- Medication Side Effects: Some of the very medications used to manage PD, particularly dopamine agonists, can cause fatigue and daytime sleepiness. Furthermore, fluctuations in levodopa levels can lead to energy crashes as the medication wears off.
- Sleep Disorders: Over 75% of people with PD struggle with sleep. Conditions like insomnia, REM Sleep Behavior Disorder (acting out dreams), Restless Legs Syndrome, and sleep apnea lead to fragmented, poor-quality sleep, which naturally fuels daytime fatigue.
- Mood and Mental Health: The link between fatigue and mood is a two-way street. Depression and anxiety, both common in PD, are powerful drivers of fatigue.
- Other Medical Conditions: It’s crucial to rule out other common causes of tiredness. Treatable conditions like anemia, thyroid issues, or vitamin deficiencies can be significant contributors.
The Vicious Cycle of Fatigue and Deconditioning
Understanding this cycle is perhaps the most empowering concept for managing fatigue. When you feel exhausted, your natural instinct is to rest and avoid activity. While this makes sense in the short term, over time, it leads to weaker muscles and reduced cardiovascular fitness—a state known as deconditioning.
Here’s the trap: when you’re deconditioned, your body has to work much harder to perform any task. This creates a greater sense of effort and exhaustion, which reinforces the belief that activity is the enemy. The less you do, the weaker you become, and the more fatigued you feel. Breaking this cycle is the key to long-term management.

A Multi-Faceted Approach to Managing Fatigue
While there’s no magic bullet for Parkinson’s fatigue, you have the power to make a significant difference. A proactive, multi-pronged approach can help you conserve energy, build stamina, and improve your quality of life.
A. Start with Your Healthcare Team
Your first step is to partner with your neurologist and primary care physician for a thorough investigation. This should include a review of your symptoms to distinguish fatigue from other issues, blood tests to rule out secondary medical causes, and an evaluation for sleep disorders. A comprehensive review of your medications is also critical to ensure they are optimized and not contributing to the problem.
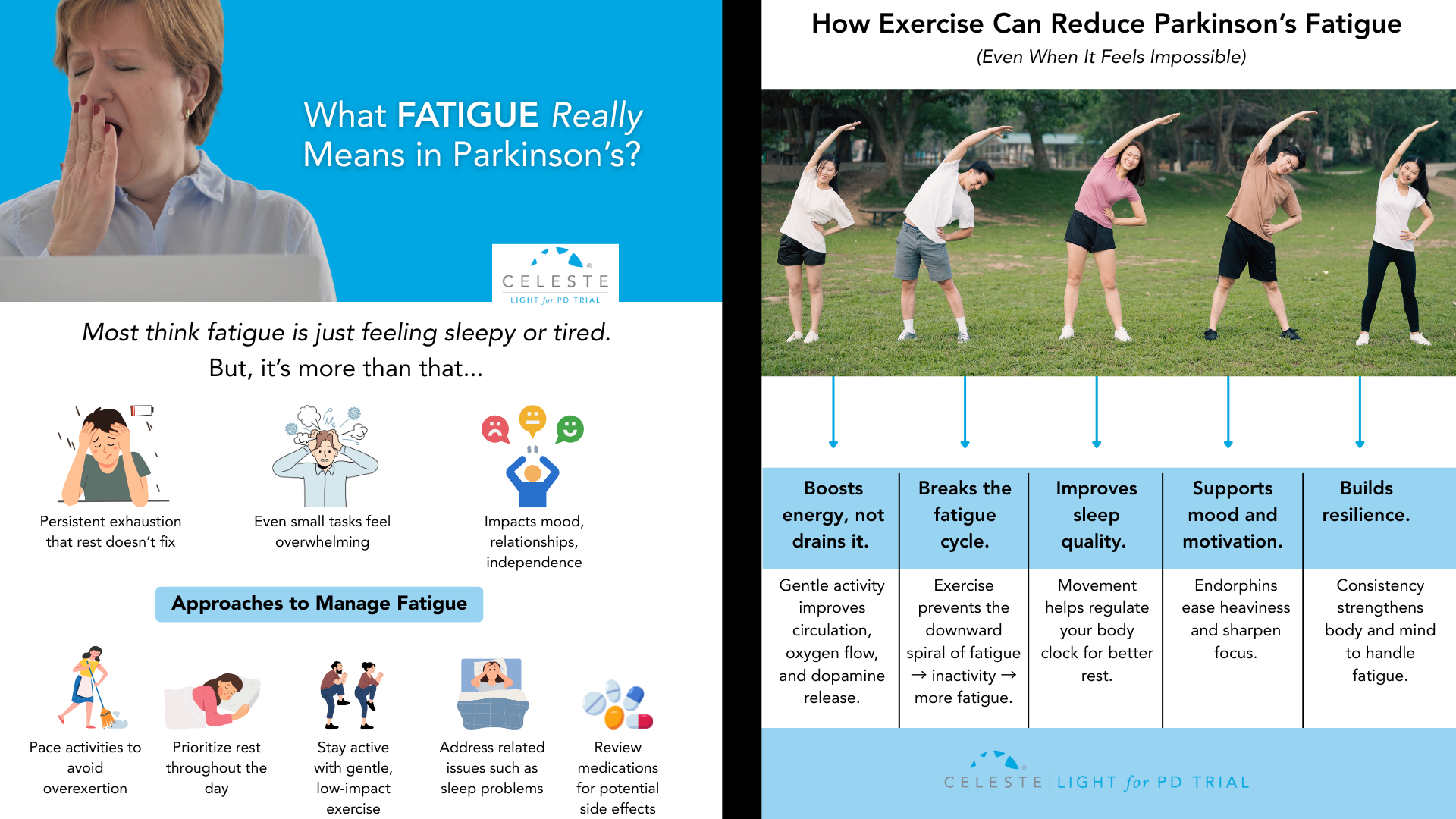
B. Movement as Medicine: Your Guide to Exercising with Fatigue
It sounds completely counterintuitive, but exercise is the single most effective, evidence-backed strategy for combating fatigue in Parkinson’s. Regular physical activity breaks the cycle of deconditioning, improves sleep, boosts mood, and helps your brain use dopamine more efficiently.
- Aerobic Activity: Aim for at least 150 minutes per week of activities like brisk walking, cycling, or swimming.
- Strength Training: Use weights, resistance bands, or your own body weight at least twice a week to rebuild muscle.
- Balance and Flexibility: Practices like Yoga and Tai Chi are fantastic for improving the efficiency of your movements.
- Getting Started: Consult a physical therapist who specializes in PD. Start slow—even 5-10 minutes counts—and gradually build up. Most importantly, find an activity you genuinely enjoy.
C. Work Smarter, Not Harder: The Art of Energy Conservation
Managing fatigue is as much about spending your energy wisely as it is about building it. The “4 Ps” are a great way to remember these strategies:
- Prioritize: Decide what must get done today and let the rest go. Focus your limited energy on what matters most to you.
- Plan: Structure your day to balance activity and rest. Schedule demanding tasks for your “on” times when you feel your best.
- Pace: This is key. Break large tasks into smaller chunks and take frequent rest breaks before you feel tired.
- Position: Sit down whenever possible for tasks like dressing or cooking. Use adaptive equipment to minimize bending and reaching.
D. Fueling for Function: The Role of Diet and Hydration
Good nutrition provides the building blocks for energy. Focus on a balanced diet rich in fruits, vegetables, and lean proteins. Avoid sugar and processed foods that lead to energy crashes. Hydration is non-negotiable—dehydration is a common and sneaky cause of fatigue. Aim for 6-8 glasses of water a day. Also, talk to your doctor about the “protein effect,” as timing your protein intake away from your levodopa doses can improve your medication’s effectiveness.
E. Rest and Recharge: Mastering Sleep and Strategic Napping
Improving your “sleep hygiene” is critical. Stick to a consistent sleep schedule, create a relaxing bedtime routine, and make sure your bedroom is cool, dark, and quiet. If you need to nap, keep it short (10-30 minutes) and take it in the early afternoon to avoid disrupting your nighttime sleep.
How to Talk to Your Doctor About Fatigue
Because fatigue is a subjective symptom, it can be hard to describe its impact to your doctor. The best way to bridge this gap is to come prepared with data. Keep a simple fatigue diary for a week or two before your appointment. Track your energy levels (on a scale of 1-10), your activities, your medication times, and your sleep quality. This transforms a vague complaint into actionable information that helps your doctor identify patterns and potential solutions.
A New Horizon in Managing Parkinson’s Fatigue
Living with Parkinson’s fatigue is an undeniable challenge, but it does not have to define your life. By understanding its roots and implementing a proactive management plan, you can take meaningful steps to reclaim your energy and engage in the activities that bring you joy.
Here at Photopharmics, we are dedicated to exploring new frontiers in managing the symptoms of Parkinson’s. We believe that innovative approaches can complement traditional therapies to address the unmet needs of the PD community.
That’s why we are pioneering the use of specialized light therapy—a non-invasive approach designed to potentially improve both motor and non-motor functions, including the pervasive fatigue that so many experience.

Our clinical trial, Light for PD, is currently underway, and it’s designed with you in mind. It’s a completely at-home trial, meaning no travel is required. Participants can use the therapy in the comfort of their own homes during their usual evening activities, like reading or watching TV.
If you are looking for new ways to manage your Parkinson’s symptoms and contribute to groundbreaking research, we invite you to learn more.
Visit lightforpd.com to see if you or a loved one may be eligible to participate in this pivotal trial. Together, we can work toward a brighter future for everyone living with Parkinson’s disease.


